STA Technical Notice: First Aid and Lifesaving Updates Following Publication of Resuscitation Council UK 2025 Resuscitation Guidelines
Posted on 15th December 2025
STA First Aid and Lifesaving Updates Following Publication of the Resuscitation Council UK 2025 Resuscitation Guidelines webinar recording delivered by Helen Done, Qualifications and Business Development Manager at Safety Training Awards, provides more detail and is available now on STA Online.
STA First Aid and Lifesaving Qualification Updates
There are no changes to STA First Aid and Lifesaving qualification learning outcomes and assessment criteria. However, STA is in the process of updating all STA first aid and lifesaving qualification resources including manuals, PowerPoints, blended learning online programmes, and where applicable, assessment strategies, tutor assessed skills sheets, multiple-choice question theory assessment papers and suggested timetables to reflect the new guidelines and industry standards.
In the meantime, STA has produced a First Aid / Lifesaving Resource Manual Addendum to support Approved Training Centres (ATCs), tutors, assessors, quality assurers and learners following the recent publication of the Resuscitation Council UK (RCUK) 2025 Resuscitation Guidelines. Its purpose is to clearly outline how the updated guidance affects the content of STA first aid and lifesaving qualifications.
The STA First Aid / Lifesaving Resource Manual Addendum is available to download from STA Online now.
The Resuscitation Council UK (RCUK) 2025 Resuscitation Guidelines will be implemented in RCUK courses from January 2026. Therefore, for any STA first aid or lifesaving courses being delivered on or after 1st January 2026, it is acceptable for ATCs to implement the technical updates within this technical notice and the resource manual addendum. However, ATCs should be aware that there will be differences in the STA first aid and lifesaving qualification course resources until the updated qualification resources are mandatory.
ATCs must use updated resources for all STA first aid and lifesaving courses starting on or after Wednesday 1st April 2026. STA will inform ATCs and relevant personnel as soon as they are available (early 2026).
During the transition period of 1st January 2026 to 31st Match 2026, learners should not be penalised if they are using techniques in line with either the latest Resuscitation Council UK (RCUK) 2025 Resuscitation Guidelines or the current STA qualification resources.
For example, if a learner performs infant CPR using the updated guidelines of a 15:2 compression:ventilation ratio with the two-thumb encircling technique, this should be deemed competent; as should a learner who performs infant CPR using a 30:2 compression:ventilation ratio using the two-finger technique.
From 1st April 2026, the Resuscitation Council UK (RCUK) 2025 Resuscitation Guidelines must be implemented by ATCs in all STA first aid and lifesaving qualification courses and all qualification resources will have been updated to align ahead of this date.
To review the full guidelines, please visit Resuscitation Council UK (RCUK) 2025 Resuscitation Guidelines.
Casualty Management and First Aid
- Use a structured first aid assessment of a person appearing ill, injured or in shock: ABCDE (A-Airway, B-Breathing, C-Circulation, D-Disability, E-Exposure)
- New guidance advises calling 999 for any unresponsive person before assessing breathing, with ambulance service call handlers supporting recognition and CPR instructions
- Airway opening for casualties with a suspected cervical spine injury always has priority over in-line immobilisation; using a jaw thrust manoeuvre should maintain a neutral position of the neck
- Place adults and children with a decreased level of responsiveness who do NOT meet the criteria for CPR into a lateral (side-lying) recovery position
- In cases of agonal breathing or trauma, do NOT move the person into the recovery position
- Slow, laboured breathing, as well as other abnormal patterns such as agonal gasping or panting, must be recognised as signs of cardiac arrest
- The four links of the chain of survival have been revised for 2025 to include recent advances in resuscitation science in prevention, dispatcher guidance, first response systems, survivor support, and recovery:

- CPR is most effective when performed on a firm surface. However, rescuers should not move a person from a ‘soft’ surface e.g. bed to the floor. Start CPR on the bed and, if needed, compress the chest deeper to compensate for the soft mattress
- Anaphylaxis – If symptoms persist five minutes after administration, give a second dose of adrenaline, ideally in the opposite leg
- Drowning: Call 999 / 112. If the casualty is awake and responsive, first aiders should stay on land and direct the casualty back to land with clear verbal and visual instructions. If possible and safe to do so, first aiders may reach out to the casualty through a flotation device, lifebuoy, rescue tube or other rescue equipment based on their confidence, competence and training to do so. If a land rescue is unsuccessful, first aiders must await further emergency assistance. First aiders must never enter the water, as they might risk drowning. If the casualty is unresponsive in the water, only in-water rescue trained rescuers should enter the water. They should provide a flotation device, lifebuoy, rescue tube or other rescue equipment. Keep the casualty’s head out of the water. Open the airway and check for breathing. If the casualty is not breathing, if feasible and safe (with an effective flotation device), they should provide 5 rescue breaths in the water as soon as possible. Retrieve the casualty to land as soon as possible. Spine immobilisation in water should not delay removing the casualty from the water when resuscitation is required. Upon exit from the water, perform a casualty assessment. If responsive, breathing and uninjured, place in the recovery position, monitor and prevent hypothermia. Be prepared to perform CPR. If unresponsive and not breathing, perform CPR for a drowning casualty. Immediately give 5 rescue breaths (or ventilations using 100% inspired oxygen if available and first aiders are appropriately trained), before starting 30 chest compressions. Deliver 2 rescue breaths. Continue consistently high-quality compressions and effective rescue breaths at a ratio of 30:2 with minimal chest compression pauses. If an AED is available, dry the chest quickly and follow the device prompts to apply and use it.
Paediatric Basic Life Support (PBLS)
- Paediatric patients are defined as persons aged 0-18 years of age. When distinguishing between age groups, e.g. for specific skills or techniques:
- Infant for neonates and children up to 1 year
- Child for children aged 1-12 years
- Adolescents for teenagers aged 13-18 years.
- When performing CPR on paediatric casualties, use a compression-to-ventilation ratio of 15:2 if trained in paediatric basic life support; otherwise, use a ratio of 30:2
- Use the two-thumb encircling method for chest compressions in infants
- Use the one-hand or two-hand technique in children older than 1 year, or when unable to give high-quality chest compressions with the two-thumb-encircling technique
- Infant choking – use the two-thumb encircling technique to perform chest thrusts as advised for chest compressions, but compressing the sternum more sharply
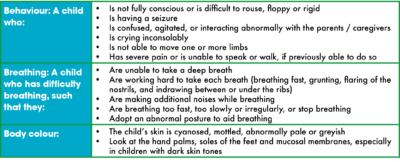
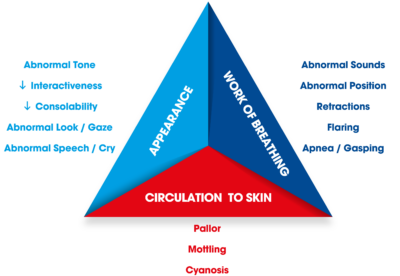
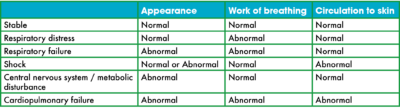
- Timely identification of critically ill children is vital for the prevention of cardiac arrest. First aiders can use triage tools such as the BBB-tool (Behaviour – Breathing – Body colour) or Paediatric Assessment Triangle (PAT) to support recognition of critical illness and injury in paediatrics:
BBB-Tool
Paediatric Assessment Triangle
Automated External Defibrillators (AED)
- Adult AED Pad placement – ensure the left pad is placed correctly around the side of the chest (not on the front) and under the armpit (not too low)

- If a casualty is wearing a bra, first aiders should prioritise correct pad placement and contact with bare skin. If this can be quickly achieved without removing the bra, then it is acceptable to keep the bra in place. There is no evidence that an underwire in a bra causes harm. If the bra interferes with correctly locating the pad position, then the bra should be removed. First aiders should not be concerned about exposing the casualty’s chest to apply the pads and should prioritise life-saving interventions

- Paediatric AED pad placement:
- The anterolateral (front and side) pad position can be used in children weighing less than 25kg when using paediatric pads, provided these do not touch each other, as contact between pads can cause charge arcing. One pad is placed below the right collarbone (clavicle) next to the breastbone, and the other on the left side under the armpit (left axilla)

- If using adult-size pads:
- Use the anteroposterior (front and back) position in infants and children weighing less than 25kg who can easily be turned onto their side for pad placement, and in casualties where the anterolateral (front and side) position is more difficult to achieve without contact between the pads. The anterior (front) pad is placed mid-chest left of centre (sternum), and the posterior (back) pad in the middle of the back between the shoulder blades (scapulae)




- Use either the anteroposterior (front and back) position or the anterolateral (front and side) for children weighing more than 25 kg and adolescents. The anteroposterior (front and back) position can be used if the pads are too big to be positioned in the anterolateral (front and side) position. If the anteroposterior (front and back) position is used in adolescents, avoid placing the pads over breast tissue
- Use the anterolateral (front and side) position in larger children, as this leads to less interruption of chest compressions than the anteroposterior (front and back) position.
If you have any questions, please do not hesitate to contact us.